Perinatal Stroke
Introducción
Neonatal stroke is estimated to occur in 1 per 2300 to 5000 live births.1 This estimate may be an underrepresentation of the true incidence of neonatal stroke because of the inherent challenges in diagnosing this condition. In the adult, stroke is defined as “rapidly developed signs of focal (or global) disturbance of cerebral function lasting greater than 24 hours (unless interrupted by surgery or death), with no apparent nonvascular cause.”2 In this definition, there is heavy reliance on the clinical signs of neurological dysfunction. These signs are not usually apparent in the neonate because motor dysfunction is not easily appreciated, and sophisticated repertoires of behaviors such as language or the ability to follow commands have not yet developed. In the newborn, symptoms are vague, including encephalopathy, seizures, hypotonia, poor feeding, and apnea. This list of symptoms may be present in many of the diseases treated in the neonatal intensive care unit; therefore, trying to ascertain which are caused by stroke can be immensely challenging.
The correct identification of stroke, however, is paramount for many reasons, ranging from identifying potentially modifiable risk factors to acute therapeutic intervention (particularly for sinus venous thrombosis). Managing long-term outcomes, which tend to be poor, is difficult but may improve with aggressive early intervention and emerging therapies such as transcranial magnetic stimulation and constraint-induced therapy.
In neonates, a proposed definition of stroke is as follows: “A group of heterogeneous conditions in which there is a focal disruption of cerebral blood flow secondary to arterial or venous thrombosis or embolization, between 20 weeks of fetal life through the 28th post-natal day, and confirmed by neuroimaging or neuropathological studies.” In this definition, there is a conspicuous absence of any clinical sign or physical exam finding suggesting neurologic dysfunction caused by stroke. As in adults, stroke in neonates can be subcategorized based on the affected vascular distribution (arterial vs venous), by whether the primary mechanism is ischemic or hemorrhagic, and by the presumed timing of the event (prenatal or postnatal). In this chapter, arterial ischemic stroke is discussed first, followed by venous stroke (better known as cerebral venous sinus thrombosis, CVST), and then hemorrhagic stroke. Prenatal and perinatal ischemic events defined by the term presumed perinatal ischemic stroke (PPIS) are also discussed.
PERINATAL ARTERIAL ISCHEMIC STROKE
Definitions
Arterial ischemic stroke occurs when an arterial vessel is occluded by a thrombus or an embolus, resulting in ischemic injury to the brain tissue distal to the occlusion. A thrombus is defined as a clot that is adherent to the wall of a vessel, whereas an embolus is a nonadherent thrombus. The embolus may be moving within arterial vessels or venous vessels or may become paradoxical by crossing from venous to arterial circulation. Paradoxical emboli may be more likely to occur in the neonate as right-to-left shunts are a necessary part of cardiovascular physiology during the transition from fetal to neonatal circulation.
Epidemiology
Perinatal arterial ischemic stroke (PAIS) is often a single lesion (70%) and is frequently located in the anterior circulation (71%). A large international cohort revealed that there is a predominance of left-sided strokes affecting the middle cerebral artery (MCA) when only 1 hemisphere is involved (51% for isolated left vs 25% for isolated right) and that bilateral strokes occur in approximately 24% of patients. The left-sided predominance often leads to language deficits and right hemiparesis.4 Seizures are a common presenting symptom and are often focal in manifestation.5 Mortality was estimated in 1 study as 18 of 134 or 13.4% (8 died of hemorrhagic stroke, 9 died from arterial ischemic stroke, and 1 died from asphyxia and sinus thrombosis).
Pathophysiology
Perinatal arterial ischemic stroke is dominated by necrosis. After 24 hours, activated microglia invade the lesion. They become foamy macrophages in 36–48 hours, and astrocytic hypertrophy develops over 3–5 days. Over the longer term, the lesion becomes gliotic as glial fibrillary processes are laid down. There may be mineralization or cavity formation over the next weeks to months. After 4 to 6 weeks, cystic evolution occurs, leading frequently to ex vacuo dilation of the ipsilateral ventricle. The ischemic penumbra is the area surrounding the focal ischemic area destined for necrosis. In the penumbra, cellular metabolism is deranged because of decreased cerebral blood flow.
Risk factors for PAIS
(see Figure
1) can be
grouped according to maternal, fetal, or placental origin;
naturally, there is great overlap among the 3 categories.
Pregnancy itself is a hypercoagulable state because of
innate protective thrombophilic factors that come into play
to protect the mother from postpartum hemorrhage. In fact,
this is true to such an extent that the maternal risk of
stroke in the 3 days postpartum is elevated 34-fold when
compared to the nonpregnant state.1 In
a normal pregnancy, there is a marked increase in the
procoagulant activity in the maternal blood, characterized
by elevation of factors V, VII, VIII, IX, X, and XII and
fibrinogen (increases 2-fold) and von Willebrand factor,
which is maximal around term. In
addition, there is a decrease in protein S activity and an
acquired activated protein C resistance, leading to less-effective
thrombolysis.
Other
maternal factors increasing stroke risk include preeclampsia3;
eclampsia; hemolysis, elevated liver enzyme levels, and low
platelets (HELLP syndrome); elevated homocysteine and 677 C
→ T mutation in MTHFR gene; factor V Leiden mutation;
chorioamnionitis; drug exposure (cocaine or amphetamine with
associated vasospasm and poor perfusion of placenta);
primiparity with a prolonged second stage of labor8;
and autoimmune diseases such as lupus with associated
autoantibodies. Fetal risk factors include birth-related
trauma, which may result in stretch injury of carotid or
vertebral arteries, leading to dissection, thrombus
formation, and subsequent stroke. Congenital cardiac disease
may lead to embolic stroke from thrombus that may occur in
the heart because of diminished flow or the presence of
right to left shunts. Cardiac surgery,9 atrial
septostomy,10 and
the presence of catheters have
been shown to increase the risk of stroke. Infection, such
as meningitis, increases the risk of stroke. Interestingly,
there is a male predominance among children with stroke, and
in neonates in the International Pediatric Stroke Study (IPSS)
registry, there were 249 with PAIS, 149 (57%) of whom were
boys.
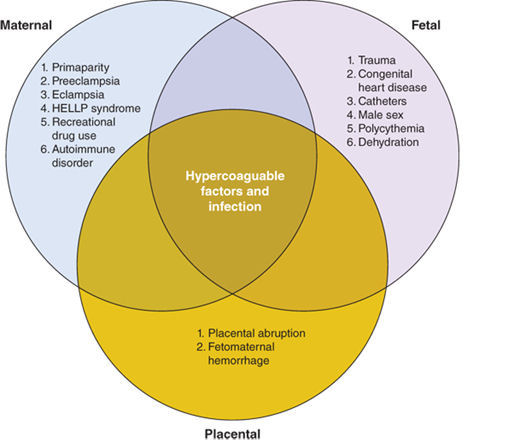
FIGURE 1
.- Risk factors associated with perinatal stroke. Hypercoagulable states and infection affect maternal, fetal, and placental categories. HELLP, hemolysis, elevated liver enzyme levels, and low platelets.
The placenta is a low-flow system, which makes it more susceptible to clotting because of stasis effects. Thrombotic lesions are often found in the placenta of those neonates diagnosed with stroke. In a paper dedicated to the role of placental pathology in neonatal stroke, Elbers described abnormal placental pathology in 10 of 12 patients with neonatal stroke (7 with arterial ischemic stroke and 5 with CVST). In these patients, 50% demonstrated thromboinflammatory processes. A further 42% demonstrated acute catastrophic events, and 25% demonstrated decreased placental reserve. Two patients had evidence of chorioamnionitis, suggesting that infection also plays an important role.
Clinical Presentation
Seizures are the most common sign of PAIS. Seizures commonly occur in the first hours or days of life and are focal and clonic5 (see Figure 2). A focal seizure in a neonate who is not encephalopathic is highly suggestive of PAIS. Stroke, however, can also be the etiology for severe encephalopathy to the extent that it is no longer uncommon to provide therapeutic hypothermia to an encephalopathic infant and later discover evidence of stroke on imaging rather than global injury caused by hypoxic ischemic encephalopathy. In a prospective cohort of 124 encephalopathic neonates, 6 (5%) were found to have focal stroke on imaging.
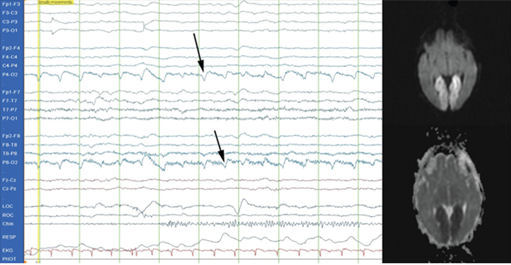
FIGURE 2.- Conventional electroencephalogram (EEG) demonstrating a typical focal seizure. This is a 2-Hz occipital seizure on the right (P4-O2 and P8-O2 leads; see arrows) that was associated with a posterior cerebral artery infarct (see magnetic resonance image).
Recognition of seizures can be challenging because of the variable clinical presentation of seizures, the complete lack of clinical correlate with many neonatal seizures, the dissociation between electrographic events and clinical events that occurs frequently after seizures are treated, and the frequent use of paralytic or sedating agents, especially during therapeutic hypothermia. A subclinical seizure is defined as one that occurs in the absence of any overt clinical repetitive or rhythmic movement that would be readily identified as seizure. In a study of 41 neonates, there were a total of 293 electrographic seizures (seizure apparent on electroencephalogram [EEG] only), 84 of which had a clinical correlate,15 thus illustrating the fact that many neonatal seizures have no clinically visible features.
In another study, 51 neonates at high risk for seizure were monitored with EEG, and 12 had a total of 526 seizures. Of these 526 electrographic seizures, only 179 or 34% had clinically recognizable symptoms when the video and EEG were reviewed simultaneously. Of the 179 seizures with clinical correlate, only 48 were recognized as seizures by care providers. Conversely, there were 129 clinical seizure-like events documented by providers that had no EEG correlate. In other words, 73% of the time, seizure-like events were incorrectly identified at the bedside as seizures.This study clearly illustrates the need to monitor with EEG not only to correctly identify true seizures but also to limit the incorrect identification of seizure-like events and inappropriate administration of anticonvulsant drugs.
Another challenge to the recognition of seizures is that treatment with anticonvulsants can cause “electroclinical dissociation.” This condition exists after administration of a drug such as phenobarbital, which may lead to the cessation of clinical seizures while electrographic seizures continue. Last, there is the unanswered question regarding whether aggressive treatment of subclinical seizures has any positive impact on developmental outcome or whether overtreatment of movements incorrectly perceived as seizures has potential adverse effect on neurodevelopmental outcome.
Because of the challenges of correctly identifying seizures, EEG monitoring should be used to identify seizures, monitor for electroclinical dissociation, and monitor the effectiveness of treatment. Conventional EEG (cEEG) is preferred because full coverage of the head using the 10- to 20-electrode placement system yields more accurate identification of the area of brain from which the seizure originates. However, cEEG is of limited utility at the bedside for non-neurology-based personnel because of the difficulty of interpreting the complex waveforms. Limited channel-monitoring devices, such as amplitude-integrated EEG (aEEG), are being used as an adjunct or in place of cEEG to improve bedside seizure detection. Although short seizures, those lasting less than 30 seconds, or those of low voltage will be missed by aEEG, it is unclear at this time whether treating these seizures is imperative or improves outcome. aEEG is capable of detecting status epilepticus, and there is no ambiguity about whether prolonged status is deleterious to the newborn brain. aEEG is easily employed by trained personnel, and if used in conjunction with cEEG, artifacts that appear seizure-like can be readily evaluated with great accuracy. The other advantage to aEEG is the ability to comment on prognosis based on the background activity, which is reassuring when there is evidence of state change in hypoxic-injured term newborns in the first 24–48 hours.
Differential Diagnosis
The differential diagnosis (see Tabla 1) for PAIS and CVST is essentially the same as for neonatal encephalopathy, a broad term used to describe a heterogeneous syndrome characterized by neurological dysfunction in the neonate. Hypoxic ischemic encephalopathy should be considered foremost for this differential diagnosis, and because of the significant overlap of symptoms, it is not uncommon for neonates with PAIS or CVST to be treated with therapeutic hypothermia. Any form of intracranial hemorrhage, including intraventricular (IVH), subarachnoid (SAH), subdural (SDH), or intraparenchymal hemorrhage (IPH), may have symptoms similar to PAIS or CVST (especially seizures and depressed mental status). Bedside cranial ultrasound can be used to quickly assess for the presence of blood.
Trauma (incidental because of birth or inflicted) must not be overlooked as a potential etiology for intracranial hemorrhage and stroke. Central nervous system infection, whether bacterial or viral (encephalitis or meningitis), may also present similarly with altered mental status and seizures and should prompt consideration of stroke. Lumbar puncture is a necessary and frequent component of the workup for these infants once imaging has been performed and the risk of herniation is deemed minimal. Hypoglycemia and electrolyte derangements (sodium, calcium, and magnesium) are treatable causes of neonatal seizures and thus should be ruled out. More uncommonly, brain tumors may present in the neonate with symptoms of neonatal encephalopathy and seizure. Mitochondrial disease, other metabolic disorders, and kernicterus should also be considered as part of the wider differential diagnosis when there is persistence of seizures and progressive alterations in mental status.
Tabla 1.- Differential Diagnosis of Stroke
-
Neonatal encephalopathy (hypoxic ischemic encephalopathy)
-
Intracranial hemorrhage
-
Intraventricular, subarachnoid, subdural, or intraparenchymal hemorrhage
-
-
Cerebral venous sinus thrombosis
-
Central nervous system infection
-
Meningitis (bacterial or viral)
-
Encephalitis
-
-
Electrolyte derangement
-
Hyponatremia
-
Hypocalcemia
-
Hypomagnesemia
-
-
Hypoglycemia
-
Metabolic diseases
-
Mitochondrial disease
-
Inborn errors of metabolism
-
Kernicterus
-
-
Tumors
-
Trauma
Diagnostic Tests
Imaging
Cranial ultrasound has a low likelihood of diagnosing PAIS.21 Computed tomography (CT) is another option, but there is higher risk to the neonate because of the significant dose of ionizing radiation, and CT may not be sensitive for infarcts that are less than 24 hours old.21 The advantages of CT, however, are the relative speed of image acquisition (several minutes) as opposed to upward of 30 minutes for magnetic resonance imaging (MRI) and could be of utility in the unstable neonate for whom redirection of care is a consideration. CT is particularly sensitive at detecting intracranial blood, but this can be achieved equally well with MRI or even with ultrasound.
The gold standard for diagnosing PAIS is MRI. This provides the highest-resolution detail regarding the extent and timing of injury. It is essential to have a basic comprehension of diffusion sequences and conventional T1 and T2 sequences when evaluating stroke. In the first 1–14 days of life (maximal in the normothermic patient by day of life 4), diffusion-weighted images (DWIs) depict areas of “diffusion restriction” as bright with “high signal intensity” compared to the surrounding noninjured brain tissue (see Figure 3, images A and E). Areas with restricted diffusion are areas where there has been injury resulting in energy depletion and failure of molecular pump machinery with subsequent decreased movement or “diffusion” of water molecules in the extracellular compartment. DWIs are compared to an apparent diffusion coefficient (ADC) map, where the areas of injury on the DWIs have areas of corresponding darkness (see Figure 3, images B and F).
After approximately 10 to 14 days,
these diffusion changes normalize, and the injury is no
longer apparent on these sequences. Care must be taken
with interpretation of diffusion images as the extent of
injury may appear greater than what is ultimately seen
on the conventional images. Pseudonormalization occurs 7
to 8 days after the injury; therefore, caution must be
used in the interpretation of diffusion imaging as the
absence of high signal intensity could represent the
absence of injury or equally that the study was
performed after day 7 or 8 when the diffusion changes
are no longer apparent.
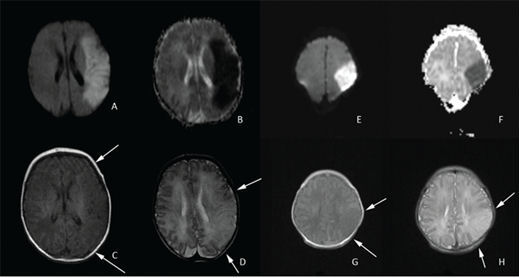
FIGURE 3
.- Diffusion-weighted and conventional magnetic resonance imaging (MRI) images of entire middle cerebral artery (MCA) distribution stroke on the left and partial MCA stroke on the right. A, hyperintensity in the left MCA distribution indicates acute MCA stroke confirmed by corresponding darkness on the apparent diffusion coefficient (ADC) map in image B. The T1 sequence shown on C reveals subtle changes in the affected area that are more prominent in the T2 sequence shown on image D (loss of cortical ribbon; see arrows). Images E (diffusion weighted) and F (ADC map) demonstrate a partial MCA territory stroke with corresponding T1 and T2 images again demonstrating subtle loss of the cortical ribbon on T1 and more apparent loss on T2 (see arrows).
The conventional T1- and T2-weighted images are useful to clarify the injury because these abnormalities should be visible on these sequences by day 7 or 8. On T1 images in the neonate, the white matter appears gray, the gray matter appears white, and the cerebral spinal fluid (CSF) is dark. Both injured cortex and injured white matter appear relatively hypointense or have “low signal intensity” (see Figure 3, images C and G) compared to normal tissue and, most important, lose the distinct boundary delineating gray vs white matter (blurring of the cortical ribbon). This change is evident from day 2 onward until the injured area undergoes cystic degeneration, at which point it appears dark like CSF. On T2-weighted images in the neonate, the white matter appears white, the gray matter appears gray, and the CSF is bright. Injured areas, including both cortex and white matter, appear relatively hyperintense or have “high signal intensity” compared to uninjured tissue, and the loss of the cortical ribbon is more evident than on T1 (see Figure 3, images D and H). This change can be appreciated from day 2 onward and is eventually replaced with bright CSF signal as the injured area undergoes cystic degeneration.
Magnetic resonance angiography (MRA) permits the evaluation of the intracranial and neck arterial vasculature. This technique is sensitive to motion artifact but may be useful to reveal underlying vessel pathology, such as dissection from birth trauma or arterial malformation. MRI and MRA are often performed with anesthesia to improve image quality by sedating the neonate so there is no movement. Wrapping techniques have been developed that employ vacuum devices to immobilize the unsedated neonate (see Figure 4), thus eliminating risk of sedation with minimal to no sacrifice of image quality.

FIGURE 4
.- Transporting the unsedated neonate. In the upper left corner, the recently fed, sleepy, and unsedated neonate has ear protection applied and then is wrapped snugly in a blanket. The blue vacuum device is then wrapped around the neonate and secured with straps. A wall suction device is then used to remove the air from the vacuum device and the neonate is immobilized. The final image shows the neonate in the appropriate size head coil ready for magnetic resonance imaging (MRI). (From Mathur et al. )
Management
Currently, the acute management of neonatal stroke is predominantly supportive. In adult stroke, normothermia, euglycemia, and permissive hypertension are accepted principles. Hyperthermia in animal models is known to increase metabolic demands if there is diminished capacity to deliver both oxygen and nutrients, leading to additional neuronal injury. In adults with stroke, hyperthermia is associated with a poorer prognosis, and in children with traumatic brain injury, hyperthermia is associated with longer hospitalization and lower Glasgow Coma Scale score. Hyperthermia has not been specifically studied in children or neonates with stroke, but based on the known adverse outcomes in adults, normothermia is a reasonable goal in the management of neonatal stroke. In the subset of encephalopathic neonates who receive therapeutic hypothermia and are subsequently found to have PAIS, one study has shown a decrease in the frequency of seizures (0/5 cooled neonates had seizures vs 7/10 with seizures who were not cooled)27 and thus suggests at least a need for future investigation into hypothermia as an intentional treatment for PAIS. Likewise, this study also suggests that treating seizures may decrease secondary neuronal injury. There is currently no evidenced-based approach to guide seizure treatment in the neonate; however, consensus seems to exist that status epilepticus (either clinical or subclinical) merits aggressive intervention18 and, depending on the institution, will often result in escalating doses of phenobarbital, followed by fosphenytoin. There is less clarity regarding the treatment of subclinical seizures, and ongoing research efforts are under way to assess this.
In terms of euglycemia, neonates do not tend to have the same elevations in serum glucose as adults because of the absence of comorbid diabetes and hyperglycemia; therefore, this tends to be less of an issue. It is important, however, to avoid hypoglycemia as symptomatic hypoglycemia in term newborns has been shown on early MRI to have an association with white matter, cortex, basal ganglia, posterior limb of the internal capsule, and thalamic injury. It is justified, then, to make a theoretical leap and assume that hypoglycemia can conceivably worsen an existing injury caused by PAIS and should therefore be avoided.
Adjunctive treatments currently investigated for hypoxic ischemic encephalopathy include xenon gas, erythropoeitin, and prophylactic use of anticonvulsant drugs, including phenobarbital, levetiracetam, and topiramate, but these are not yet being studied clinically for PAIS. Neonates are not usually treated with aspirin or antiplatelet drugs. On a case-by-case basis, particular disorders of hypercoagulability or cardiac diseases with large clot burden have been treated with either low molecular weight heparin (LMWH) or heparin drip. In one report, 3 neonates were discovered to have aortic arch thrombosis and were successfully treated with LMWH.
With respect to the workup of neonatal stroke, it is essential to obtain MRI of the brain and vasculature and is reasonable to consider echocardiogram in the context of congenital heart disease and to perform Doppler ultrasound to evaluate flow. The hypercoagulable workup may be deferred from the acute setting, in which values are often reflective of the pregnancy state rather than intrinsic abnormalities of the neonate. The mother, especially in a first pregnancy, should have a hypercoagulable workup that includes examination of antiphospholipid antibodies and anticardiolipin antibodies. The neonate as part of outpatient follow-up can receive routine testing, including for antithrombin III, protein C, protein S, activated protein C resistance, factor V Leiden mutation, prothrombin gene mutation (G20210A), and antiphospholipid antibodies.
Outcome and Follow-up
Cerebral palsy (CP) is defined as a static, predominantly motor, deficit that results in spasticity in the extremities because of upper motor neuron injury of the cortical spinal tract. Of 36 infants with arterial stroke, 58% had CP,30 and other estimates of motor deficit after stroke range from 30% to 40%. Injury to the internal capsule (motor fibers), Broca’s area/Wernicke’s area (language centers), or basal ganglia or a large stroke (greater than two-thirds the area of a major vessel) are correlated with an increased risk of CP.30 Types of CP include spastic (about 80%), ataxic (about 10% caused by damage of the cerebellum), and athetoid/dystonic (10% to 20% with a mixed picture of hyper- and hypotonia because of injury of basal ganglia and corticospinal tracts). MRI is a useful tool for prognosis, and in 37 neonates with stroke, 7 (19.4%) developed unilateral spastic CP (hemiplegia) and had pre-Wallerian degeneration changes evident on MRI that were predictive of this outcome. In those who did not develop CP, 27 of 29 patients had no measurable change in the internal capsule or cerebral peduncle, which are components of the descending corticospinal tract. In another study of 14 neonates with PAIS, diffusion-weighted MRI signal was abnormal in the descending corticospinal tract of 10, and this correlated well with motor outcomes.
With respect to cognitive function, a recent study examined cognitive performance in 18 neonates at 12 and 24 months following stroke. At 12 months, children scored significantly below the normative sample on the Bayley Psychomotor Development Index and at 24 months significantly below the normative sample on both the Bayley Mental Development Index and the Psychomotor Development Index. There were no differences found in this small sample based on stroke type (PAIS vs CVST) or based on which hemisphere was affected. A study of 26 older children also with unilateral stroke found that when tested at age 3.5 years and then again at almost 6 years, there was little difference among preschool-aged children when compared to normal controls. However, school-aged children (particularly males) had impaired performance on Full Scale IQ Working Memory and Processing Speed but not on Verbal IQ or Performance IQ. This suggests a trend toward later emergence of deficits reflective of dysfunction in higher levels of cognition and the potential need for ongoing educational support and assessment.
CEREBRAL VENOUS SINUS THROMBOSIS
Definition
Cerebral venous sinus thrombosis occurs when a venous sinus, deep vein, or cortical vein is completely or partially obstructed by thrombus. This may occur without measurable parenchymal injury when there is incomplete occlusion of the vessel or good collateralization (blood flows out of the affected area through alternate routes) or may be associated with venous infarct. The term bland infarct is used to denote an infarct that does not have secondary hemorrhage. Typically, venous infarcts accompany 40% to 60% of CVSTs, and in one study, 29 of 69 neonates (42%) had infarct associated with CVST. In this same study, secondary hemorrhagic conversion of the venous infarct was a frequent finding seen in 24 of 69 neonates (35%), whereas in another study of 109 neonates, 38% of infarcts remained bland and 62% became hemorrhagic. Blood is not limited to the confines of the infarct as there is also frequent intraventricular and extraparenchymal hemorrhage (28% and 26%, respectively, in the Moharir study).
The anatomical distribution of infarct is different in CVST compared to PAIS. In PAIS, the injured area is attributable to a lack of blood flow in a known arterial territory. In CVST, the findings of injury do not correspond to arterial territories, but predictable patterns are seen based on the areas drained by the affected sinus. For instance, with a straight sinus thrombosis, there may be evidence of injury to unilateral or bilateral basal ganglia and thalami, whereas with sagittal sinus thrombosis, there may be evidence of injury in a parasagittal watershed distribution.Hemorrhagic lesions have been reported with the following associations: thalamo-ventricular hemorrhage with internal cerebral vein occlusion, bilateral thalamo-ventricular hemorrhage with vein of Galen occlusion, striato-hippocampal hemorrhage with basal vein thrombosis, temporal lobe or cerebellar hemorrhage with transverse sinus thrombosis, or temporal lobe hemorrhage alone with vein of Labbe thrombosis.
Epidemiology
The incidence of venous ischemic stroke is estimated at 0.41 to 0.67 per 1000 live births, with most recent estimates ranging from 2.6 to 12 per 100,000. CVST is being diagnosed with increasing frequency because of greater clinical awareness of the disease and imaging techniques that are more sensitive. Mortality estimates range from 6% for CVST36 to perhaps as high as 19%,40 depending on the study and in which country it was done.
Pathophysiology
Venous infarcts occur because of the obstruction of cerebral veins by thrombus, which results in localized edema with pathologic evidence of swollen vessels and neurons with ischemic damage. Petechial hemorrhages occur that may coalesce into larger areas of hemorrhage. There may also be external mechanical factors, such as compression of the sagittal sinus from skull bones caused by molding or positioning, that confer a higher risk of venous thrombus formation because of interference with one or more of the components of Virchow’s triad and result in hemodynamic flow changes, such as stasis, endothelial injury, and liberation of hypercoagulable factors.
The superior sagittal sinus is affected most frequently (62%), followed by the lateral sinuses (39%), then the straight sinus (30%), then the internal cerebral vein (10%), vein of Galen (8%), cortical veins (3%), and finally the jugular vein (1%). In Moharir’s study, 80% of neonates had multiple-sinus involvement. Risk factors for CVST are multiple and like PAIS can be divided on the basis of maternal, fetal, or placental origin with natural overlap between these categories (see Figure 1).
Maternal risk factors are known to include premature rupture of membranes, chorioamnionitis, gestational diabetes, and preeclampsia with associated endothelial dysfunction. Fetal risk factors include acute systemic illness, polycythemia, and dehydration. A difficult delivery with or without trauma to the skull and injury to superior sagittal sinus has also been associated with increased risk of CVST; hypoxic ischemic encephalopathy is present in as many as 20% of cases later found to have CVST. Male neonates have an increased frequency of CVST, but the underlying reason for this is unknown. Referring to the IPSS registry, of 92 neonates identified with CVST, 68 were male (74%).35In the Berfelo study, 75% of those with proven CVST were male. In a 2004 paper, Golomb hypothesized that the size of the male infant (which at term is slightly larger than the female) may contribute to the increased risk.
Given that the inciting factor in this mechanism of stroke occurs because of the presence of clot, it is essential to evaluate the neonate (and mother) for the presence of a hypercoagulable state. In children, prothrombotic disorders are present in one-to two-thirds of patients with CVST. In neonates, however, the frequency of prothrombotic states seems lower, with one study showing 3 of 15 (20%) neonates with abnormalities, including 2 with (MTHFR) mutations and 1 with factor V Leiden mutation. Assessment of antithrombin III, protein C, protein S, factor V Leiden, and prothrombin 20210A gene mutation is standard. MTHFR, homocysteine level, and lipoprotein (a) should also be evaluated. In a larger study of 52 neonates with CVST, 29 of the 52 were tested for antithrombin III, and all tests were normal.
In this same study, 32 of 52 were tested for both protein C and S levels, and all tests were normal. Forty-one of 52 were tested for G1691A factor V Leiden mutation, and a mutation was present in 2. The G20210A prothrombin gene mutation was tested in 18 of 52 and was present in 2. MTHFR C677T and A1298C mutations were tested in 23 and present in 13, but interestingly, all 23 had normal homocysteine levels. Anticardiolipin antibody, lupus anticoagulant, prothrombin time (PT), partial thromboplastin time (PTT), and fibrinogen should not be overlooked. It is also critical to ensure that the results obtained are compared to age-adjusted normal controls. At this time, there is no consensus regarding the optimal timing of these studies and whether results from the acute period vs several months later are more reflective of the true state of coagulation.
Clinical Presentation
In CVST, seizures are often the presenting sign. In a study of 52 neonates, 29 or 55.8% presented with seizures that developed at a median time of 1.5 days. In the Moharir study,36 seizures occurred in 69% and encephalopathy in 53%. A term infant with intraventricular blood, thalamic hemorrhage, and seizures has a common triad suggestive of venous sinus thrombosis. Other presentations include lethargy, a full fontanelle, and prominent scalp veins. As in PAIS, the next most common findings are apnea, temperature instability, hypotonia, poor feeding, and encephalopathy. Encephalopathy can be further defined as inappropriate level of consciousness, lack of spontaneous activity, low tone, absence of primitive reflexes, and autonomic dysfunction, including tachycardia or apnea.
Differential Diagnosis
For information on differential diagnosis, see the section on PAIS and Table 1.
Diagnostic Tests
Ultrasound findings in the
term neonate with intraventricular and thalamic hemorrhage,
especially if the patient has had clinical seizures, should be
considered highly suspicious for CVST. In
the hands of experienced technicians and radiologists with color
Doppler ultrasound, it is possible to view the sinuses clearly
and diagnose absent flow, which is consistent with CVST.
Computed tomography without contrast may show linear hyperintensities in places consistent with venous structures, suggesting the presence of thrombosis. On a CT scan with contrast, the term empty delta sign is used in the context of suspected CVST. This term refers to the pattern of thrombus evolution within the triangular-shaped sagittal sinus (the delta sign) that may appear to have a central hypointensity (the empty part of the delta). If imaging occurs within the first several days or after 2 months, this sign is not likely to be present. It also only applies to the sagittal sinus and can easily be missed if the thrombus does not extend into the posterior third of the sinus. This sign is not reliable in neonates because of the tendency for physiologic polycythemia in conjunction with the normal hypomyelinated neonatal brain to mimic the empty delta sign.
Magnetic resonance imaging with magnetic resonance venogram (MRV) is the preferred method for diagnosing CVST because of the lack of exposure to harmful radiation and the sensitivity of the technique. On MRI, in the subacute stages, the thrombus will appear hyperintense on T1-weighted images (see Figure 5, image D).
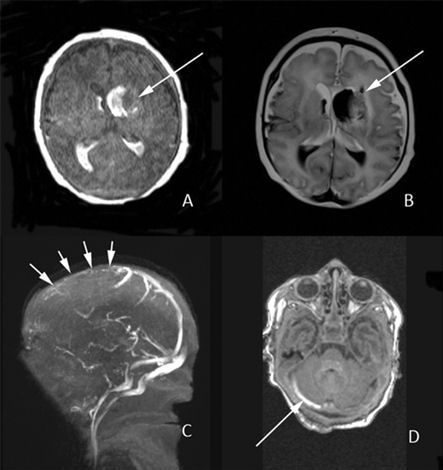
FIGURE 5.- Cerebral venous sinus thrombosis. Image A is a T1 sequence showing hyperintense blood within both lateral ventricles as well as extension into the parenchyma at the left frontal pole of the lateral ventricle. The T2 sequence in image B displays more clearly the intraparenchymal extension of hemorrhage (see arrows). This hemorrhage is the sequelae of a cerebral venous sinus thrombosis (CVST). C, Magnetic resonance venogram (MRV) with occlusion of the anterior portion of the superior sagittal sinus indicated by absent flow (no hyperintense signal seen near arrows). D, T1 image with right transverse sinus thrombosis. Careful interpretation of this finding must be made as thrombus can easily be confused with subdural blood in this location.
MRV should be obtained simultaneously because, in the acute phase, the thrombus is likely to appear isointense on T1 and hypointense on T2; this could be easy to misinterpret as normal flow. MRV is a study with images dedicated to evaluation of the venous structures and is the most effective at delineating areas where flow is absent (see Figure 14-6, image C). If there is an associated infarct, diffusion imaging techniques will reveal this. Infarcts that are notconfined to known vascular territories or those that are bilateral and involve deep gray nuclei should prompt suspicion for CVST and acquisition of MRV sequences. Hemorrhage is frequently associated with CVST (see Figure 5, images A and B) and can be seen on MRI with susceptibility-weighted images (blood appears black with blooming artifact; see Figure 6, images E and F). In one study of 67 neonates who had full imaging data, an infarct or hemorrhage was present in 66%. Serial imaging is required if a clot is present in order to evaluate for extension or propagation, in which case treatment is recommended (see section on management). EEG monitoring for seizures and a hypercoagulable workup as described for PAIS should be undertaken in the case of CVST.
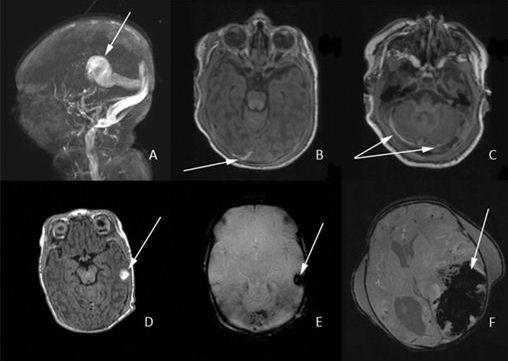
FIGURE 6.- Intracranial hemorrhage: A, Magnetic resonance venogram (MRV) of a vein of Galen malformation with widely dilated venous system. B, T1 image with subdural hemorrhage (SDH) shown in the right occipital lobe (see arrow). C, SDH in the posterior fossa (see arrows). Note the similarity to image D in Figure 7. Image D reveals a small left-sided intraparenchymal hemorrhage (IPH) caused by a presumed cortical vein thrombosis that is characteristically hyperintense on T1. Image E shows this same hemorrhage with blooming artifact on a susceptibility-weighted image (SWI). Finally, image F shows a massive left-sided IPH (blood is dark on SWI) with midline shift, leading ultimately to herniation in this unfortunate neonate.
Management
Appropriate supportive care, such as correcting dehydration and treating infection and seizures if present, is undisputed in the literature on CVST. Unlike many conditions affecting the neonatal central nervous system, CVST is unique in that there is the potential for treatment with anticoagulation. Previous studies have shown that untreated CVST results in greater than 50% of patients having adverse outcomes with cognitive and motor impairments and epilepsy in 46% to 79%. If associated infarct and seizure exist, outcome tends to be even worse,35 thus heightening the urge to treat. In this context of urgency, however, current clinical guidelines do not align with respect to whom to treat. Recommendations in 2008 from the American Heart Association suggest considering anticoagulation in selected neonates with severe thrombophilic disorders, multiple cerebral or systemic emboli, or clinical or radiological evidence of propagating clot. The recommendations from the American College of Chest Physicians (also in 2008) are more inclusive and recommend treating CVST when there is no extensive intracranial hemorrhage and to consider treating when clot is propagating even in the presence of extensive hemorrhage.
In one retrospective study, 43 of 81 neonates with CVST were treated.46 Fourteen received unfractionated heparin(UH), 34 received LMWH, 2 were treated with aspirin, and 1 received warfarin. There were no treatment-related adverse outcomes, and in the treated infants, clot propagation occurred in only 1 after LMWH was discontinued at 49 days. In a prospective study, Moharir enrolled 104 neonates with CVST, 53 of whom received anticoagulation therapy as either UH or LMWH.36 Anticoagulation was initiated at diagnosis in 41 (39%) neonates and after thrombus propagation was discovered on serial MRI in 12. In the treated group, there were no anticoagulant-related deaths or extensive systemic hemorrhage during the period of anticoagulation. There were 14 neonates with significant pretreatment hemorrhage who were anticoagulated, and none experienced worsening hemorrhage. One of 41 (2%) treated neonates experienced thrombus propagation, whereas 14 of 47 (30%) of untreated neonates experienced thrombus propagation. Clinically, propagation was silent in all but 1 neonate, who presented with worsening seizures, but new venous infarction was documented in 6 of 15 with clot propagation (40%). Outcomes for those with clot propagation were unfavorable (death or any neurologic deficit at last follow-up) in 10 of 15 neonates.
Repeat MRI and MRV are often obtained 5 to 7 days after the first studies to evaluate whether clot propagation is occurring. Serial Doppler ultrasound studies may detect a propagating thrombus. Full recanalization was demonstrated in 89% by 3 months.36 Among other variables, intracranial hemorrhage, propagation of thrombus, and anticoagulant use did not predict the severity of neurodevelopmental outcome.
Outcome and Follow-up
With respect to developmental outcomes in the Moharir study, the mean follow-up was 2.5 years, and of those 85 neonates who survived, 35 were normal, 12 had mild deficits, and 38 had moderate-to-severe deficits. Deficits ranged from sensorimotor deficits, to receptive and expressive language problems, to cognitive and behavioral concerns. Seizures were present in 69% at the time of diagnosis, and epilepsy was documented in only 18% of survivors.
In another study, DeVeber found that 77% of neonates followed to 1.6 years were “normal,” but this finding applied to the group of children and neonates as a whole and was not analyzed by treatment. Long-term outcome in 1 study with only 9-month follow-up was notable for 45% being “uncomplicated” and a severely abnormal outcome in 19% of survivors. It is clear that more studies are needed to better delineate outcomes, with particular emphasis on studying outcome as affected by treatment with anticoagulation.
HEMORRHAGIC STROKE
Definitions
There are 5 major, clinically relevant types of intracranial hemorrhage in the neonate: SAH, SDH, IPH, cerebellar hemorrhage, and IVH.48 Intra-axial blood is defined as blood within the brain or within the ventricle; hence, this category includes IPH, cerebellar hemorrhage, and IVH.
Extra-axial hemorrhage is by definition blood outside the brain parenchyma and is named according to the location of blood compared to the surrounding meninges. This category includes SAH and SDH. IVH in the term newborn is pathologically distinct from IVH in the preterm newborn, which is discussed elsewhere in this text. IPH, SDH, and SAH commonly occur in term newborns, whereas IVH and cerebellar hemorrhage tend to occur in prematurely born infants.
With more frequent use of MRI, cerebellar hemorrhage is increasingly diagnosed in preterm infants. This is important as the incidence is highest in those born weighing less than 750 g, for whom there is a 17% incidence of cerebellar hemorrhage according to the largest reported series. In one small study of 15 preterm infants (median gestational age 25 weeks and 2 days and median birth weight 730 g), 13 experienced “notable, otherwise unexplained motor agitation in the days preceding the diagnosis” of cerebellar hemorrhage.50 Cerebellar hemorrhage is associated with adverse developmental outcomes, including neuromotor disability, expressive and receptive language deficits, as well as socialization and behavioral abnormalities.
Epidemiology
The true incidence of intracranial hemorrhage in the full-term newborn is likely underestimated. When 101 asymptomatic term newborns were examined with MRI within the first 72 hours of life, 46 of them (46%) had SDHs and 20 of these (43%) also had hemorrhage in the posterior fossa. In a study of 53 full-term symptomatic neonates with intracranial hemorrhage, all had both intra-axial and extra-axial hemorrhage. SDH was present in 50/53 (94%), whereas SAH was only present in 8/53 (15%). Associated IVH was seen in 12/53 (23%). In this same study, 13 of 53 neonates died or had care withdrawn based on the severity of the hemorrhage and poor prognosis indicated by EEG, yielding a mortality rate of 24.5%.
Pathophysiology
Infrequently, neonatal intracranial hemorrhage is the result of a vascular defect. The 2 most common defects are aneurysms and arteriovenous malformations. Intracranial hemorrhage related to aneurysm rupture is often characterized by rapid neurologic deterioration and SAH that may be later identified by MRI and cerebral angiography as secondary to aneurysm. Arteriovenous malformation is most commonly encountered in the context of a vein of Galen malformation (which is more likely to present with high-output congestive heart failure) (see Figure 6, image A). With this malformation, the hemorrhage is likely to be intraparenchymal or intraventricular.
Intracranial hemorrhage is more often associated with risk factors related to the delivery rather than vascular defects. SDH and IPH are more often the result of prolonged or precipitous delivery, vaginal breech delivery, instrumental delivery (forceps or vacuum assist), primaparity, or extreme multiparity. According to a large retrospective study of greater than 500,000 deliveries, the risk of intracranial hemorrhage (including SDH, IPH, IVH, or SAH) with vacuum assist is estimated to be 1 in 860 compared to 1 in 1900 of those neonates who were delivered vaginally without use of the vacuum device. With forceps delivery, the ratio is increased to 1 in 664 for intracranial hemorrhage. If both forceps and vacuum assist are employed, the ratio further increases to 1 in 256. For cesarean section, the ratio is 1 in 907 for cesarean delivery performed after trial of labor. With failed attempt at “operative delivery,” which is either vacuum assist or forceps, the rate for cesarean section increases to 1 in 334. In summary, there is an incremental increase in the frequency of intracranial hemorrhage if more than one surgical technique is employed. The mechanism of injury caused by birth-related factors is likely because of mechanical stress from elongation of the head and subsequent stretching of the falx and tearing of the tentorium. The venous sinuses are exposed to these same mechanical forces and can also be ruptured.
Risk factors other than the mode of delivery include thrombocytopenia, vitamin K status, and deficiency of coagulation factors. Intracranial hemorrhage is a rare complication of each of these diseases. Thrombocytopenia was present in 11 of the 50 neonates in the Brouwer study, and low platelet levels (less than 150 × 109 L-I) were more commonly seen in those who died. In another retrospective study, 2 of 23 neonates with intracranial hemorrhage were found to have thrombocytopenia.54 Neonatal isoimmune thrombocytopenia occurs in 0.2 per 1000 live births, and cranial imaging should be part of the management of these infants so that this rare complication is diagnosed.
Vitamin K administration at the time of birth is now considered standard of care, but vitamin K status must not be overlooked as a possible etiology for intracranial hemorrhage. Treatment of mothers with phenobarbital, coumadin, aspirin, or antituberculosis drugs may indirectly cause vitamin K deficiency in the newborn, subsequently increasing the risk of intracranial hemorrhage. In one case report, a mother treated with 100 mg of phenobarbital daily for seizures gave birth to a term infant via vaginal delivery with vacuum assist; the infant subsequently developed a large left hemispheric SDH.
Clinical Presentation
Hemorrhage occurs because of rupture of veins, and blood accumulates in the various spaces described previously. If this occurs in the posterior fossa around the cerebellum, increased intracranial pressure may result because of blockage of the cerebral aqueduct as well as mass effect from the blood itself. Clinical symptoms can include a tense or bulging anterior fontanelle, increasing head circumference, lethargy, apnea, and bradycardia. Urgent imaging and consideration of neurosurgical intervention are required. Later complications of intracranial hemorrhage can include hydrocephalus caused by CSF outflow obstruction or difficulty with resorption of CSF at the level of the arachnoid granulations (communicating hydrocephalus). Shunting may be required if this occurs.
As in the case of PAIS or CVST, intracranial hemorrhage presents with seizures the majority of the time (72%). In one study, with temporal lobe hemorrhage particularly, there was an association with apneic seizures and a further 10 infants (19%) presented in this manner, thus bringing the total with seizure as the presenting sign to 91%. The other 5 infants in the study were admitted because of perinatal asphyxia, respiratory distress, and development of posthemorrhagic ventricular dilation. Seizures in the context of intracranial hemorrhage can be challenging to treat, as evidenced by the fact that 12 of 53 infants in this study needed 2 anticonvulsant drugs and another group of 18 required 3 anticonvulsant drugs.
Differential Diagnosis
For information regarding a differential diagnosis, see the section on PAIS and Table 1.
Diagnostic Tests
Cranial ultrasound can be readily used at the bedside to identify IPH, which appears as a homogeneous area of increased echogenicity. CT scan without contrast is extremely sensitive to the presence of blood products, but the adverse effects of ionizing radiation are undesirable. MRI of the brain is the gold standard for evaluating intracranial pathology in the neonate both from a safety perspective and for obtaining the most accurate information. If blood is present, on the conventional images it will appear hyperintense on T1-weighted images (see Figure -6, images B and D) and hypointense or black on T2-weighted images. The appearance of blood can be easily remembered by the fact that blood signal is the opposite of the corresponding CSF signal in that sequence. Susceptibility images or gradient echo (GRE) sequences can be used to demonstrate the presence of blood products (see Figure 7, images E and F) and is as sensitive as CT scan.
Management
Much of the management of intracranial hemorrhage is supportive. Serial imaging and sequential neurological examination in the asymptomatic newborn is an appropriate approach. If, however, a large lesion is present or if there are signs of increased intracranial pressure or brainstem compromise, then neurosurgical evaluation is acutely necessary. In the Brouwer study, 3 of 21 infants with significant midline shift needed craniotomy for evacuation of hematoma. In another study, 5 of 24 infants with intracranial hemorrhage required surgical intervention.
Thrombocytopenia should be corrected if present. If vitamin K is deficient, this also should be addressed as well as any other coagulopathy. In both the acute and chronic phases of the illness, daily head circumference should be measured to monitor for posthemorrhagic hydrocephalus. In the Brouwer study, 16 infants developed hydrocephalus, 6 of whom needed subcutaneous reservoirs and 3 of those 6 went on to convert from reservoir to ventriculoperitoneal shunt.
Outcome and Follow-up
Of the 40 surviving infants in the Brouwer study, 37 were seen in follow-up at a mean age of 20 months.52 The mean developmental quotient (DQ) was 97, and there was no difference among groups based on neurosurgical intervention. Only 1 infant developed epilepsy and 3 developed CP. There are few long-term studies evaluating outcome; therefore, although one can be cautiously optimistic, data are not available.
PRESUMED PERINATAL ISCHEMIC STROKE
Definitions and Mechanism
Much research has focused on acute, symptomatic stroke in the neonate that commonly presents with seizures. There is, however, increasing interest and research in stroke that is asymptomatic in the newborn period and later diagnosed by asymmetric early motor development or early hand preference. Presumed perinatal ischemic stroke (PPIS) is defined as occurring in a neonate over the age of 28 days with a normal perinatal neurologic history who develops neurologic deficits attributable to a remote focal infarction confirmed on neuroimaging performed later in infancy. PPIS, like acute stroke in the term neonate, can be subdivided based on the vascular territory affected: arterial vs venous. The vast majority of PPISs (80%) seems to affect arterial territories, and most are in the MCA distribution.
This type of stroke is referred to as APPIS to emphasize the arterial distribution. As with PAIS, the implied mechanism is thrombotic or embolic, but interestingly, unlike PAIS, for which congenital cardiac disease plays a more prominent role, of 15 children with PPIS who were evaluated by echocardiogram, none was found to have clinically significant structural or functional abnormalities. In contrast, when venous structures are affected, the term periventricular venous infarction (PVI) is used. The mechanism is suspected to be related to fetal germinal matrix hemorrhage, with the mass effect of this hemorrhage on the nearby medullary veins causing subsequent infarction.
Hemorrhagic stroke can also occur prior to birth and has been described in families with early handedness and a history of porencephaly (a fluid-filled cavity in the brain communicating with the ventricles). This disease is termed familial porencephaly and has been linked to a mutation in the COL4A1 gene, which encodes the α1 chain of type IV collagen. The α1 chain binds with 2 α2 chains, and this heterotrimer becomes a crucial component of the basement membrane of blood vessels forming a “sheet-like network beneath the endothelium and surrounding smooth muscle cells.”
Because of early research in a mouse model, it was thought that there was an interaction between this autosomal-dominant genetic predisposition and the environment, as mouse pups born via surgical delivery did not have the same intracranial hemorrhage burden as those born vaginally.61 In humans, there seems to be a wide phenotypic spectrum, ranging from preterm infants born with resolving hemorrhage60 to adults who have migraine headache, nephropathy, and tortuosity of the retinal vasculature, thus making it challenging to define a relationship between genetics and the environment. Consideration should be given to genetic testing for the COL4A1mutation in the following circumstances: preterm infants who develop atypical IPH and all infants who are born with porencephalic cysts.
Epidemiology
In a retrospective analysis of 59 children with PPIS, 63% were male. Typically, PPIS has been described in infants who were born at term; however, there is also emerging data on PPIS in the preterm infant, with as many as 15% of those known to have PPIS having been born before 37 weeks’ gestation.
Clinical Presentation
Early hand preference, particularly in the first 12 months of life, is likely pathologic and should prompt neuroimaging with MRI of the brain. Of the 59 children studied by Kirton et al, 44 presented with early hand preference. Seizure is the next most frequently occurring symptom, with 10 of 59 or 17% presenting this way. When the APPIS group was compared to the PVI group, a pattern emerged, with the majority of PVI patients (92%) presenting with motor asymmetries, whereas the APPIS group had a much higher likelihood of presenting with a seizure (25% for APPIS vs 0% for PVI). The explanation for this may relate to the fact that the cortex, the epileptogenic component of brain tissue, is injured with APPIS but not with PVI. The median age in Kirton’s study for parental concern of motor asymmetry was 5 months. Physician concern was raised by a median of 7 months and diagnosis made eventually by a median age of 12 months.
Diagnostic Tests
The emphasis in the diagnosis of PPIS is on the remoteness of the injury; hence, there cannot be evidence of acute injury, and diffusion-weighted MRI images are therefore of no utility. On conventional images from MRI, there should be evidence that indicates chronicity of the injury, with features such as encephalomalacia, gliosis, and atrophy (see Figure 7, images C and D). MRI must have the following features to diagnose PVI: unilateral periventricular white matter infarction in a medullary vein territory (see Figure 7, image B) with 4 or more of focal periventricular encephalomalacia, T2 prolongation in the posterior limb of the internal capsule, cortical sparing, hemosiderin within the lesion, germinal matrix or ventricle, and relative sparing of the basal ganglia.
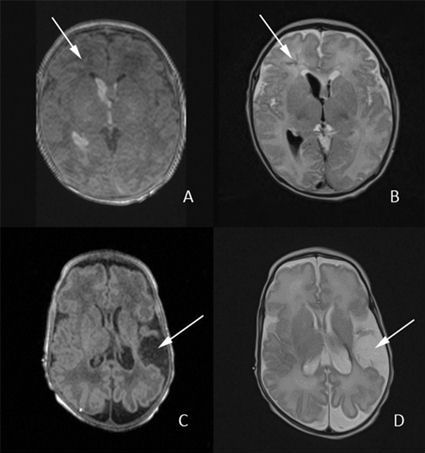
FIGURE 14-7.- Presumed perinatal ischemic stroke: A, T1 image demonstrating hyperintense intraventricular hemorrhage in both ventricles (right greater than left). There is a subtle hint of pathology in the right frontal white matter that is clearly seen on the accompanying T2 image (image B; see arrows), with dark-appearing linear structures that may correspond to clotted vessels. This injury is presumed caused by compression of the medullary veins in this right frontal area and is termed a PVI or periventricular venous infarction. C and D, T1 and T2 images, respectively, of arterial presumed perinatal ischemic stroke (APPIS); these demonstrate the typical findings of chronicity of injury with encephalomalacia (see arrows) as the only evidence remaining of this in utero event.
Outcome and Follow-up
In a retrospective study of 22 children diagnosed with PPIS at a mean age of 6 months, 21 of the 22 (95%) had clinically significant hemiparesis.58 Twelve of the 22 (55%) had speech, cognitive, or behavioral deficits.58 Five of 22 developed persistent seizures, 1 with infantile spasms.58 In a larger study of 59 children, which included the 22 children just discussed, 87% were described as having a poor outcome, with 82% having motor disability and 42% having epilepsy.
Management
There is no acute management involved in the diagnosis of PPIS, but nonetheless it is important to identify stroke as the etiology so that early intervention with supportive services such as physical therapy, occupational therapy, and speech therapy can be employed.
SUMMARY
Stroke in the neonate is common, and with better detection through clinical awareness and the use of appropriate imaging modalities, better long-term outcomes in this group of infants can be achieved.